
Weekly Roundup: Consensual Delusions And A Medicine Too Dangerous For Refugees Edition

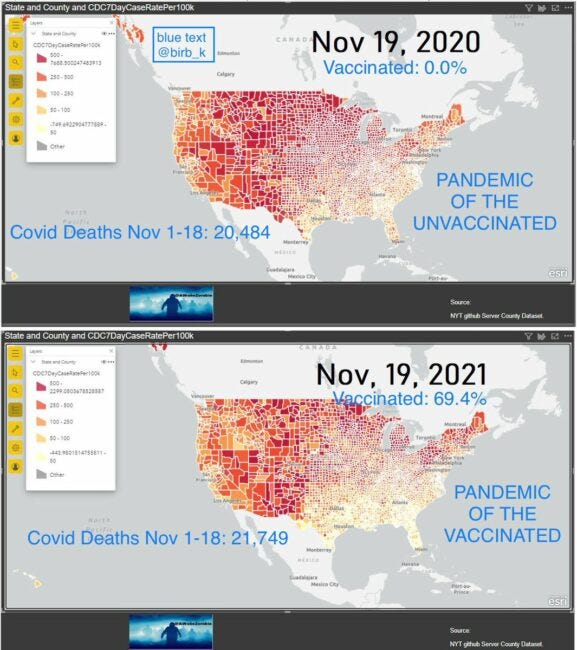
220,000 Americans dead. If you hear nothing else I say tonight, hear this. Anyone who's responsible for not taking control — in fact, not saying, I take no responsibility, initially — anyone who is responsible for that many deaths should not remain as President of the United States of America. --- Joe Biden, final debate for the Presidential election, 2020
Well, we're at 800k now and rising -- or are we? Put on your most logical, bloodless, thoughtful hat, and let's consider a dangerous question together: Why don't Africans die of COVID-19? Fewer than 100,000 Africans have died from the virus since the beginning, even though there are more than 1.2 billion Africans and about 350 million... well, let's not say "Americans", let's say "residents of the United States".
Complain all you want about American health care, but it's better than African health care, or at least that's what I'm told by every African with whom I've ever spoken on the topic. On the whole, Africa is about seven percent vaccinated, compared to many places in America where the vaccination rate is eighty percent or higher. What about mask-wearing, hand-washing, social distancing, and all the repugnant COVID theater that provides the control freaks of the Western world such unprecedented opportunities to dictate how others live? Do you suppose they do more of that in Africa, or less?
Do they even have a Dr. Fauci, the American superhero who has saved so many of us?
Given that African-Americans are at statistically higher risk of dying from COVID-19 than their non-PoC counterparts, why are African-Africans so unaffected? After almost two years of taking the ostrich approach, the medical community is starting to really think about this. My Blue Tribe readers will no doubt be flabbergasted to learn that a coalition of African doctors thinks that the widespread use of ivermectin for other illnesses in Africa might have stymied COVID-19 infection vectors. Ivermectin? Isn't that the Joe Rogan horse paste for stupid hicks in trailer parks?
Naturally, I have a theory of my own -- but first, let's talk about why international refugees, another group of people with a suspicious immunity to death-by-covid, aren't getting their vaccines.
Before we do, the usual disclaimer: The staff here at Riverside Green is always at least one booster ahead of the normies. We firmly believe that the vaccine is safe and effective for adults, children, infants, animals, and fish. In order to write for this website, you must affirm that you are at least triple-vaccinated and willing to wear a double mask in your car. We fucking love science, especially when that science is explained to us on television.
Whew. Glad that's over.
If you are an American or European, you have no doubt heard that the vaccines are safe and effective. Our social media performs a very sophisticated OCR on every image posted and will automatically insert a scolding disclaimer to any picture with certain key words in it, telling you that the vaccines are safe and effective.
The vaccines are so safe and effective that a coalition of concerned scientists (the best kind, really) filed an FOIA request to get more information about vaccine testing and rollouts, just to reassure those "vaccine-hesitant" trailer-park types who are busy eating horse paste. These requests are normally filled within 20 days, but in this case we are going to have a slight delay of... 55 years. By 2076, we should all have the information on how safe and effective the vaccines are.
Nothing to worry about, of course. The FDA wouldn't approve the vaccine for 5-year-olds if there were any problems whatsoever.
Since it's unfair that American 5-year-olds are getting their THE JABS ahead of elderly people in other countries, the United Nations has decided to purchase a massive number of vaccines for the refugees of the world... but there's one little problem: the vaccine makers won't sell to the UN. Roll the tape:
Gavi, which operates COVAX with the World Health Organization (WHO), says that where those applying for doses, mainly NGOs, can't bear legal risks, deliveries from that stockpile can only be made if vaccine-makers accept liability. . The companies that are willing to do so under these circumstances provide only a minority of the programme's vaccines, according to people familiar with the matter and the documents, written by Gavi staff for a board meeting starting at the end of November.
Four firms have agreed to accept liability for vaccine side effects: the three major Chinese providers plus Johnson&Johnson. If that list sounds familiar, it's because that's also the list of THE JABS that apparently do absolutely nothing against Omicron. The private-company mRNA shot vendors, by contrast, want nothing to do with the legal consequences of vaccinating refugees.
Perhaps the firms don't have Instagram accounts and therefore aren't aware just how safe and effective the jabs are?
Not to worry; refugees are remarkably resilient to COVID-19. The last number I saw suggested that fewer than 30,000 refugees have died of COVID, out of a cohort estimated at 26-plus million. One in a thousand, basically. Not quite the African ratio of one in twelve thousand, but better than the US-resident ratio of one in 400 or so.
Now, if you're one of those repugnant nationalist types, you probably think this is because most "refugees" are military-age men in excellent health who left their women and children behind to face hell while they zip off to a new life in Europe or America, secure in the fact that they can easily replace their women and children with native equivalents in their new country. That is, of course, completely false... except where it's completely true, of course.
Gosh, in some places it's absolutely true.

We know, of course, that men ages 18-24 are all but immune to COVID, as shown below:

So this explains why refugees aren't at much risk for COVID. It doesn't explain why the vaccine manufacturers are so worried about offering THE JAB to them.
The above chart might also explain why Africa is such a "cold spot" for COVID deaths; the age distribution in what they called "The Dark Continent" in the astoundingly racist world of my youth is far, far younger than what we have in America or Europe. The chances of dying from COVID as an 85-year-old in Africa are very low, because the chances of being alive in the first place at that age are very low. Simple as that.
I wouldn't spend too much time looking at that COVID-by-age chart, by the way; it could produce crimethink if you peruse it too carefully. You might start to wonder why we need to inject five-year-olds with a substance that is literally considered too dangerous for refugees, just to protect cohorts of people who are going to die of something anyway. This is an astounding inversion of human practice throughout history. Remember "Women and Children First!" on the Titanic? If that happened in 2021 and we treated it like we treat COVID, we'd shove the kids out of the way to get 90-year-olds on the lifeboats. I know a surprising number of people who are vaccinating their schoolchildren for the express purpose of protecting their parents or grandparents; this line of thinking produces a profound disquiet in my heart.
While I don't want you to look at the above chart too long, I do want you to look at it for a moment, then look at this one:

I doubt any of my readers will be surprised by the fact that the vast majority of deaths in this country occur among old people, in pretty much the same ratio as COVID-19 deaths. The age-stratified graphs for heart disease and cancer look remarkably similar to COVID-19 charts.
The next question: How do you know when someone has died of COVID-19? Sometimes it's obvious, but most of the time it's a case of people dying with COVID-19, perhaps a little faster than they would have died otherwise. It is perfectly acceptable in America to code a death as COVID-related even if it is not the primary cause of death. Doing so entitles the care facility to reimbursement under CARES. The most rabid Blue Tribe "fact checkers" do not seriously dispute this.
(It's worth noting that Facebook's attorneys recently characterized their much-vaunted "fact-checking" infrastructure as opinion-based only.)
The CDC allows and even encourages the reporting of COVID-19 as a cause of death when it is not the primary cause of death; see the guidelines here.
Knowing everything we know above, let's go through some hypotheses as to why the United States has the highest COVID-19 death rate in the world and African countries are among the lowest, taking refugee infection rates into account as well. I'll put them approximately from most insane to least insane, by my reckoning anyway:
Hypothesis Zero: Africans and refugees are genetically resistant to COVID-19. This seems unlikely, not least because African-Americans are more likely to die from COVID-19 than non-Black Americans or Africans. And refugees are ethnically diverse, to say the least.
Hypothesis One: Ivermectin and other effective low-cost treatments are more popular elsewhere in the world because they are not in the grip of a pharma-governmental complex. This one has a little more traction in my mind, because it is a fellow-traveler of other exceptionally American conditions due to powerful pharma influence, like the opioid crisis and the extremely slow decision to take Vioxx off the market. The use of alternative COVID-19 therapies is commonplace elsewhere in the world but considered to be the sign of crackpot racist insanity in the United States; there is a wildly popular and front-page-listed subreddit devoted to crowing over the deaths of Covid patients who try other treatments, for example.
Hypothesis Two: COVID is almost exclusively a disease of old people, and we live in an old-person country.. This one stands up pretty well until we look at the discrepancies between the United States and other aging countries. In a very real sense, there are two categories of COVID death rates in the world. The first category is the United States and the United Kingdom, both of which regularly top the charts for reported deaths. The second category is... everyone else, from devil-may-care Sweden to ultra-authoritative China, both of which report a fraction of our death rate despite wildly different approaches to treatment and prevention. So we'd have to come up with a supplemental hypothesis to account for that.
Hypothesis Three: Death rates from COVID are pretty much universal around the world, but since the disease has become highly politicized in the United States and United Kingdom there are different and more enthusiastic standards for both testing and reporting. This one is my favorite, because it requires zero "leap of faith" assumptions. We know that the US and UK use aggressive standards to list COVID as a cause of death. We know that hospitals are financially encouraged (in the US) and bureaucratically encouraged (in the UK) to list COVID as a cause of death. We know that the US media positively delights in politicizing COVID deaths. We know the UK has a strong authoritarian tradition that has informed its COVID policy from Day One.
Admittedly, I'm personally inclined to like this final hypothesis because it lines up with my personal worldview that many of the world's perceived problems are produced by the combination of poor data management and sensationalist media coverage. Is COVID-19 a real disease? Of course it is. Is it deadly? Certainly. Is it an historically unprecedented pandemic with a unique power to kill people? Probably not. But it is in the interest of various and diverse entities to pretend so.
Example: Forbes just ran a headline stating 7 Deaths From Omicron Covid-19 Coronavirus Variant In UK, Showing It’s Not The ‘Omicold’. Sounds reasonable; seven people have died in just two weeks! However, influenza by itself accounts for 25 deaths a week in the UK! The combination of influenza and pneumonia, which is the method by which COVID-19 kills most people without heart conditions, kills five hundred people a week in the UK. Seven deaths in two weeks? By that standard, Omnicron isn't just "the common cold"; it's far less deadly than the common cold. But the headline is, strictly speaking, true -- and it's being repeated in one form or another across the UK media.
More than ever, we are living in the era of the consensual delusion. For the purposes of this article, I define a "consensual delusion" as "an idea or concept that can be readily disproven, or credibly challenged, via reliable public information, but which is nevertheless widely believed and acted upon by the general public." I'd like to list some American consensual delusions for you here, along with the evidence that refutes them, but doing so would be effectively fatal to my ability to feed and house my son. If you have a reasonable IQ, a reasonable education, and no emotional disorders, you already know what they are, from your own observation. If you lack one or more of those qualities listed above, you'd just get violently agitated if I discussed any of our society's cherished illusions, so let's not bother.
COVID-19 has reached the status of consensual delusion in America. This doesn't mean it hasn't killed anyone, because it has. It has killed people close to me, even. For all I know, it will kill me next week; I'm now slouching towards the high-risk cohorts. But I could just as easily die on a commercial flight next week, and that wouldn't make commercial flights the biggest killer in America.
I spent much of the past three weeks in California, observing the most rabid of the consensual delusionists up close. You can't eat a meal indoors in LA County without producing acceptable documentation of vaccination. This is the same Los Angeles that has seen murders and violent crimes increase significantly during 2021, the same Los Angeles where homeless encampments prevent kids from walking to school, the same Los Angeles where organized gangs are, ahem, acquiring goods en masse without police intervention. None of this has the attention of the government. It's all COVID, all the time. While lane-splitting on various motorcycles I was flabbergasted at the number of people I saw wearing two masks while sitting alone in their cars. This is dangerously close to mental illness and is indistinguishable in practice from "making signs" to "ward off the Devil".
The real tragedy is that, as Curtis Yarvin and others have noted, it would have been easy to contain COVID-19 in the beginning. All you had to do was shut down international travel. The virus is barely transmissible on hard surfaces and it doesn't survive long. We didn't do that, because to do so would have damaged our other cherished consensual delusions, from some poppycock about human rights to the belief that people who travel for leisure are morally superior to people who just sit in their trailer park and read Industrial Society and Its Future. Trump was absolutely pilloried for attempting the mildest variant of such a policy. COVID-19 is the most important thing in the world -- but it's not more important than the uninterrupted flow of cheap labor into the Western World and the equally uninterrupted flow of pleasure tourism out of it.
The UNHCR has gone some way to consider the impact of COVID-19 on refugees. Their conclusion? COVID-19 didn't do much to refugees -- but the policies put in place to contain COVID-19 have been devastating. If you read the UNHCR report in its entirety, you'll get the sense that the coronavirus isn't that big of a deal. It's the response to the coronavirus that has been deadly and will continue to haunt us for the foreseeable future.
Hypothesis Zero: the UNHCR is correct.
Hypothesis One: in this regard, we are all refugees.
* * *
For Hagerty, I wrote about an old boss and an imaginary truck.